
Reflective Models Explained: How to Use Them Properly

Reflective models help professionals evaluate their experiences, improve their practices, and meet regulatory requirements. In healthcare, reflection is essential for maintaining high standards of care and meeting revalidation needs, such as the Nursing and Midwifery Council's (NMC) requirement for five written reflections every three years.
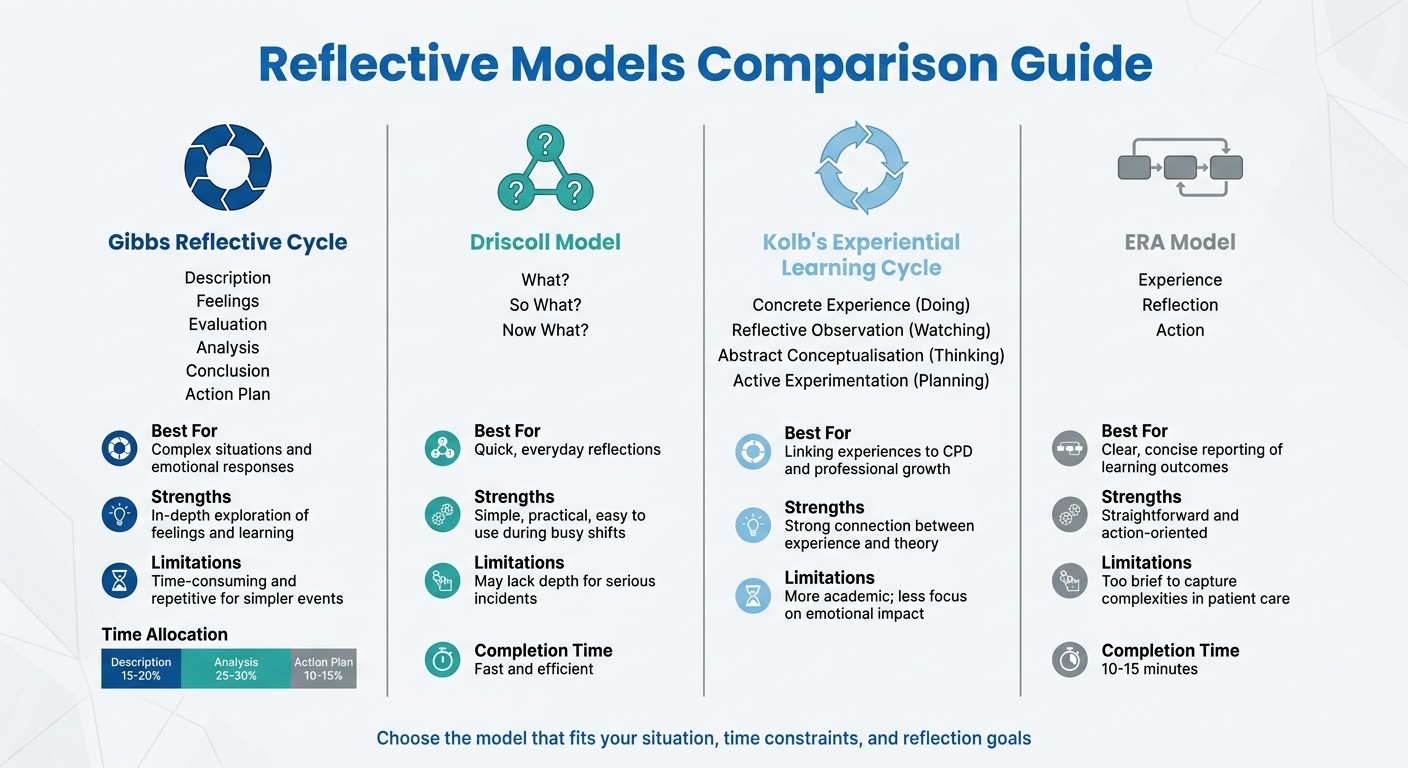
Here’s a quick overview of four popular reflective models and how they’re used:
- Gibbs Reflective Cycle: A detailed six-step process (Description, Feelings, Evaluation, Analysis, Conclusion, Action Plan) ideal for analysing complex situations and emotional responses.
- Driscoll Model: A simple three-question approach (What?, So what?, Now what?) for quick reflections, especially in fast-paced environments.
- Kolb's Experiential Learning Cycle: A four-stage loop (Concrete Experience, Reflective Observation, Abstract Conceptualisation, Active Experimentation) that connects practical experiences to learning and planning.
- ERA Model: A concise three-step process (Experience, Reflection, Action) designed for brief, actionable reflections.
Each model has its strengths depending on the situation. For instance, Gibbs is great for in-depth analysis, while Driscoll is better for quick, straightforward reflections. Kolb works well for linking theory to practice, and ERA is perfect for short, focused entries. Choosing the right model ensures your reflections are meaningful and meet professional standards.
Models of reflection for reflective writing
sbb-itb-a476a38
Gibbs Reflective Cycle
In 1988, Professor Graham Gibbs introduced the Gibbs Reflective Cycle, a six-stage framework designed to guide reflective practice. These stages - Description, Feelings, Evaluation, Analysis, Conclusion, and Action Plan - are particularly useful in healthcare, as they incorporate emotional aspects of clinical work, which play a key role in sound decision-making.
Here’s a breakdown of the six stages:
- Description: Focuses on recording the facts - who was involved, what happened, where it occurred, and when it took place.
- Feelings: Encourages you to document your emotional reactions. In healthcare, emotions are considered part of professional data, as they can influence decisions.
- Evaluation: Involves assessing the situation objectively, identifying what went well and what didn’t.
- Analysis: Takes a deeper dive into why the event unfolded as it did, linking it to clinical guidelines or relevant theories.
- Conclusion: Allows you to summarise what you’ve learned about your practice or environment.
- Action Plan: Outlines specific steps to take in similar situations in the future, such as attending training or adopting new techniques.
Gibbs highlighted the importance of reflection with this statement:
"It is not sufficient simply to have an experience in order to learn. Without reflecting upon this experience it may quickly be forgotten, or its learning potential lost."
This structured method not only improves clarity in reflective writing but also supports professional growth and compliance with revalidation requirements.
How to Apply Gibbs Reflective Cycle in Healthcare
Imagine a scenario where a nurse’s handover fails to clearly communicate a critical medication change.
- Description: You’d document the objective details, such as the handover taking place at 19:30 on a busy medical ward, involving you and two colleagues, and concerning a 68-year-old patient whose anticoagulation dose was adjusted earlier that day.
- Feelings: Here, you might note feeling rushed and anxious, possibly due to staff shortages and a 20-minute delay.
- Evaluation: While the standard handover procedure was followed, you might recognise that the medication change wasn’t adequately highlighted, even though other critical details were effectively communicated.
- Analysis: This stage might involve examining factors like stress, the lack of a structured handover tool, or fatigue from a long shift, linking these to the NMC Code’s focus on effective communication and patient safety.
- Conclusion: You might conclude that using a structured approach like SBAR (Situation, Background, Assessment, Recommendation) could have prevented the issue.
- Action Plan: A concrete step could be: "By 15th June 2026, I will complete the trust’s SBAR training module and implement this framework in all future handovers."
A common pitfall in using this framework is spending too much time on the Description stage. To ensure your reflection meets the critical thinking and professional development standards for revalidation, aim for a balanced allocation of effort: about 15–20% on Description, 25–30% on Analysis, and 10–15% on your Action Plan. This approach ensures your reflection is both insightful and actionable.
Driscoll Model of Reflection
In 1994, John Driscoll refined Borton’s framework into a straightforward three-question model: What?, So what?, and Now what?. This approach simplifies the reflective process into three clear stages, making it manageable and easy to apply.
The model moves through three main phases. The What? phase is all about describing the event - what happened, what actions you took, who was involved, and whether the experience was positive or negative. Then comes So what?, which dives into analysis, asking you to reflect on your reactions, emotions, and whether the situation aligned or conflicted with your values - personal or professional. Finally, Now what? focuses on identifying lessons learned and outlining specific steps for improvement.
One of the biggest advantages of this model is its simplicity. The University of Edinburgh highlights this by stating:
"The simplicity of this model is both a great strength and a possible limitation. It is very easy to remember and can be applied to any field or experience."
This simplicity means you’re more likely to use it regularly, whether during a shift or afterwards, helping you build strong reflective habits. It works well for both reflection-in-action (thinking on your feet during a situation) and reflection-on-action (looking back on an event later). While Gibbs’ six-stage model offers a more detailed analysis, Driscoll’s three-step approach is a quicker, more focused alternative.
For professional revalidation, the Driscoll model ensures your reflections go beyond just describing events and lead to actionable insights. It aligns with requirements like the Nursing and Midwifery Council’s five written reflective accounts, the General Pharmaceutical Council’s annual CPD records, or the General Medical Council’s appraisal portfolio. The key is to avoid lingering too long on the What? stage and instead prioritise the So what? and Now what? stages, where meaningful learning and growth occur. This structure allows for efficient documentation and immediate application of lessons learned.
Using Driscoll for Quick Reflection
Thanks to its straightforward nature, the Driscoll model is especially handy for quick reflections in fast-paced clinical environments. It’s perfect for documenting brief but impactful moments, like a medication discussion with a colleague, a near-miss incident, or an unexpected patient interaction. These short reflections, when captured promptly, can play a significant role in professional growth.
To meet regulatory standards, focus on specific trigger questions rather than just summarising events. For example, under What?, you might ask: "What went wrong last time?" or "What surprised me the most?" For So what?, consider: "How did others respond?" or "Did this challenge my values?" And under Now what?, get practical - ask, "What do I need to know for next time?" or "How will I approach this differently?".
When creating an action plan in the Now what? stage, ensure your steps are clear and actionable.
"The more often you reflect on previous actions, the more your knowledge, skills and confidence to reflect in the moment will improve."
– Caroline Needham, The Pharmaceutical Journal
For pharmacist prescribers, this model can help justify prescribing decisions and pinpoint areas for clinical development. Nurses, who must complete 35 hours of CPD over three years - including at least 20 hours of participatory learning - can also use the Driscoll framework to efficiently document both planned and unexpected learning experiences.
Kolb's Experiential Learning Cycle
Kolb's cycle provides a dynamic framework for turning experiences into meaningful learning opportunities. David Kolb’s model is built on the principle that "Learning is the process whereby knowledge is created through the transformation of experience". Unlike approaches that focus solely on reflecting after an event, Kolb’s cycle emphasises a continuous loop of doing, observing, analysing, and planning.
The cycle unfolds in four stages. Concrete Experience is the hands-on "doing" phase - this could involve performing a clinical task, attending a workshop, or dealing with a complex patient case. This is followed by Reflective Observation, the "watching" phase, where you take a step back to review what happened, identifying any gaps between expectations and reality. Next is Abstract Conceptualisation, the "thinking" stage, where you interpret your reflections to develop new ideas or refine your understanding. Finally, Active Experimentation is the "planning" phase, where you apply your new insights in practice.
This approach is particularly useful for healthcare professionals, as it helps turn isolated experiences into ongoing professional growth. The University of Hull Library highlights that "Kolb shows how reflection on an experience leads the individual to form concepts about that experience, and to be able to generalise from one experience to another". However, for the cycle to be effective, all four stages must be completed.
Kolb’s model also aligns well with professional revalidation requirements. For instance, the Nursing and Midwifery Council (NMC) requires five written reflections that connect CPD activities to professional standards [3,8]. Similarly, the Royal College of Nursing points out that "Reflection helps us to think about, plan and deliver high quality and safe care to our patients/clients". Kolb’s structured process ensures reflections go beyond simple descriptions, fostering genuine learning and improvement.
Using Kolb's Model for Professional Development
Consider how Kolb’s cycle can be applied in practice. A pharmacist prescriber used the model while managing Simon, a 50-year-old patient with high blood pressure (160/95 mmHg). During Reflective Observation, they noted that baseline renal function tests were missing, even though Simon was keen to start medication. In the Abstract Conceptualisation phase, they referred to NICE guidelines and determined an ACE inhibitor was unsuitable without these tests. For Active Experimentation, they decided on a calcium channel blocker (amlodipine) and arranged follow-up blood tests and an ECG.
When planning your own CPD, begin with a specific event, feedback, or educational activity as your Concrete Experience. During Reflective Observation, ask questions like, "What was particularly challenging?" or "What did I approach differently this time?" In the Abstract Conceptualisation stage, connect your experience to professional standards, linking it to the four themes of the NMC Code: Prioritising people, Practising effectively, Preserving safety, and Promoting professionalism.
The final stage, Active Experimentation, is where reflection turns into action. Set specific goals, such as using the SBAR tool consistently during handovers or reviewing updated clinical guidelines. The Royal College of Nursing advises that "any reflective account needs to explain what you learnt from the CPD activity, feedback or experience; how you changed or improved your work as a result, and how this is relevant to the Code". This step ensures that your insights lead to measurable improvements in patient care.
For pharmacist prescribers completing annual revalidation with the General Pharmaceutical Council, Kolb’s cycle is invaluable for documenting both planned learning (like training courses) and unplanned learning (such as near-miss incidents or difficult consultations). As Caroline Needham writes in The Pharmaceutical Journal, "a skilled reflective practitioner will develop the ability to draw on reflective practice automatically and use it as a tool to enhance interpersonal effectiveness during patient encounters". Regularly engaging with the full cycle helps embed reflection into daily practice, supporting both revalidation and improved clinical decision-making.
The ERA Model
The ERA model, introduced by Melanie Jasper, simplifies the process of reflection into three main stages: Experience, Reflection, and Action. Designed with healthcare professionals in mind, this framework offers a practical way to reflect regularly without spending too much time on documentation. As the University of Cambridge explains, "the cycle shows that we will start with an experience... This will allow us to think through the experience, examine our feelings about what happened and decide on the next steps".
The process begins with Experience, which refers to a specific clinical event, patient feedback, or a CPD activity. Following this, the Reflection stage involves breaking down what occurred, exploring your feelings, and identifying lessons learned or areas where your knowledge could improve. Finally, the Action phase is where you determine concrete steps, such as adopting a new clinical approach or confirming that your existing methods are effective.
One reason ERA stands out in healthcare is its speed and adaptability. Bradford VTS describes it as a "fast but genuinely reflective" tool that can typically be completed in just 10–15 minutes. It works well for both "reflection-on-action" (after an event) and "reflection-in-action" (during patient interactions), allowing you to evaluate your thought process in real time. This efficiency makes ERA a valuable tool for maintaining reflective practice throughout the revalidation cycle, supporting professional development without adding unnecessary administrative work.
For revalidation, ERA’s simplicity is particularly helpful. The Nursing and Midwifery Council (NMC) requires five written reflections over three years, and ERA makes it easier to meet this requirement while keeping documentation manageable. Below, we’ll explore how to use ERA effectively for brief yet meaningful reflections.
How to Use the ERA Model
ERA’s straightforward structure makes it easy to incorporate into clinical documentation. Start by recording the Experience in a concise and factual manner - what happened, when it occurred, and who was involved. In the Reflection stage, take a moment to slow down and dig deeper. Bradford VTS points out that "writing slows you down in a productive way, forcing you to probe thoughts and feelings more carefully than you ever would in your head". Focus on what was particularly challenging or what you handled differently.
The Action stage is where professional growth takes centre stage. Here, you outline how the experience has influenced your practice. For NMC revalidation, the Royal College of Nursing recommends ensuring your reflections address what you learned, how your actions changed, and how this ties into the Code’s four themes: Prioritise people, Practise effectively, Preserve safety, and Promote professionalism and trust. This approach not only meets revalidation standards but also supports ongoing improvements in clinical practice.
To streamline the process, consider starting with the Action and Reflection sections before adding a brief summary of the Experience. For an even more comprehensive approach, the "ERA+" variation includes a Review stage to evaluate whether your planned actions were successful.
Aim to use ERA for regular, short entries in your professional portfolio rather than leaving reflections until the end of a placement or revalidation cycle. Pay special attention to challenging moments, as these often provide the richest learning opportunities. During reflective discussions required for revalidation, share your entries to facilitate peer feedback and gain fresh perspectives.
Choosing the Right Reflective Model
Comparison of Four Reflective Models for Healthcare Professionals
No single reflective model works for every situation. The best choice often depends on factors like how much time you have, the complexity of the event, and what you want to achieve from the reflection. As the Royal College of Nursing puts it:
"Reflection is a conscious effort to think about an activity or incident that allows us to consider what was positive or challenging and if appropriate plan how it might be enhanced, improved or done differently in the future".
By understanding the strengths and limits of different models, you can pick the one that best suits your needs. Below, we’ll explore how various models perform in different scenarios.
For incidents that are emotionally charged, Gibbs Reflective Cycle is particularly helpful. Its six stages guide you through a thorough examination of feelings, making it an excellent choice for formal CPD logs or when it’s essential to understand what went wrong. However, its detailed approach can feel repetitive and time-consuming when applied to routine clinical tasks.
If you’re short on time and need a quick, straightforward reflection, Driscoll's "What? So What? Now What?" model fits the bill. It’s easy to recall and works well during busy shifts, particularly for the written reflections required for NMC revalidation. That said, it may not dig deep enough to analyse serious incidents or complex issues. This model is best seen as a complement to more detailed reflective practices when dealing with critical events.
For reflections tied to training or skill-building, Kolb's Experiential Learning Cycle stands out. It bridges hands-on experience with theoretical learning, making it a strong choice for CPD activities where showing how you’ve applied new knowledge is key. On the flip side, Kolb’s approach can feel academic and might not focus enough on the emotional aspects of an experience.
Beginners often find the ERA model - Experience, Reflection, Action - a good starting point. Its simple three-step structure is ideal for planning future improvements and aligns well with revalidation requirements. However, its simplicity can sometimes miss the finer details of complex care situations.
To meet revalidation standards effectively, it’s important to adapt your reflective approach based on the situation at hand.
Reflective Models Comparison Table
Here’s a quick comparison of the key features, strengths, and limitations of each model:
| Model Name | Stages/Steps | Best For | Strengths | Limitations |
|---|---|---|---|---|
| Gibbs Reflective Cycle | Description, Feelings, Evaluation, Analysis, Conclusion, Action Plan | Complex situations and emotional responses | Encourages in-depth exploration of feelings and learning | Time-consuming and repetitive for simpler events |
| Driscoll Model (What?) | What?, So What?, Now What? | Quick, everyday reflections | Simple, practical, and easy to use during busy shifts | May lack depth for serious incidents |
| Kolb's Learning Cycle | Concrete Experience, Reflective Observation, Abstract Conceptualisation, Active Experimentation | Linking experiences to CPD and professional growth | Strong connection between experience and theory | More academic; less focus on emotional impact |
| ERA Model | Experience, Reflection, Action | Clear, concise reporting of learning outcomes | Straightforward and action-oriented | Too brief to capture complexities in patient care |
Using Reflective Models for Revalidation
Reflective models provide a structured way to approach revalidation, supporting both professional growth and meeting regulatory requirements. To ensure compliance, you’ll need to document your learning using a reflective model that aligns with regulatory standards while safeguarding patient confidentiality. For example, NMC registrants are required to complete five written reflective accounts over a three-year period, using the official template provided by the regulator. These accounts then form the foundation for a mandatory discussion with another NMC-registered professional, which can take place either in person or via video call. This process not only satisfies regulatory obligations but also contributes to your professional development.
The content of your reflections is just as important as the format. The Royal College of Nursing outlines the key elements of a strong reflective account:
"Any reflective account needs to explain what you learnt from the CPD activity, feedback or experience; how you changed or improved your work as a result, and how this is relevant to the Code".
By explicitly linking your reflections to professional standards, you transform a simple record into evidence of meaningful professional growth.
Maintaining patient confidentiality is crucial in reflective documentation. The NMC emphasises this point:
"Be careful not to record any information which may identify another person".
To ensure confidentiality, use pseudonyms like "Patient A" or "Service User X", and avoid including specific dates or identifiable locations. This principle also applies to your reflective discussion partner - ensure their PIN, email, and address are stored securely. Choosing the right reflective model can make this process more effective. For instance, Gibbs’ model is ideal for detailed analysis, while the ERA model works well for quicker reflections. Tailoring your approach ensures your documentation captures valuable insights while meeting regulatory standards.
Different regulatory bodies have their own requirements. HCPC registrants must maintain a continuous and up-to-date record and may face random audits during registration renewal. The GMC advises at least 50 hours of CPD annually, with evidence documented in appraisal portfolios that include feedback and audits. To stay on top of these requirements, consider scheduling monthly updates to your portfolio to avoid a last-minute rush. If writing feels like a barrier, voice notes or bullet-point summaries can be a helpful starting point before formalising them into the required format. Regular portfolio updates not only ensure compliance but also reinforce ongoing professional development.
Conclusion
Gibbs, Driscoll, Kolb, and ERA each bring their own strengths to reflective practice. Whether it’s Gibbs’ detailed breakdown for analysing complex or emotional situations, Driscoll’s straightforward focus for routine reflections, Kolb’s connection between experience and planning, or ERA’s concise, action-focused insights, each model offers something valuable. For example, Gibbs’ Reflective Cycle is ideal for creating in-depth revalidation accounts, while Driscoll’s model excels at keeping reflections simple and to the point. The key takeaway? These models help transform everyday experiences into meaningful learning that improves patient care.
Beyond enhancing reflective practice, these tools also support compliance with professional standards. Structured reflection isn’t just about meeting regulations - it’s a way to grow professionally. Using a consistent model ensures reflections are thorough and insightful, moving past surface-level descriptions. This approach helps practitioners clearly demonstrate what they’ve learned, how their practice has evolved, and how their experiences align with professional codes. Ultimately, it’s about keeping your practice focused on patients while meeting regulatory requirements.
FAQs
Which reflective model should I use for this situation?
When selecting a reflective model, consider how complex the situation is and how comfortable you are with reflective practices. If you're dealing with a straightforward scenario, the ERA cycle - which focuses on Experience, Reflection, and Action - is an easy-to-follow choice. For situations that require a deeper analysis, Gibbs' Reflective Cycle offers a more structured framework, guiding you through six detailed phases. Ensure your chosen model meets the expectations of professional bodies such as the NMC, HCPC, or GMC, depending on your field.
How do I write reflections that meet NMC revalidation standards?
To meet the NMC revalidation requirements, you’ll need to write five reflective accounts over a three-year period. These accounts should centre on experiences such as Continuing Professional Development (CPD) activities, feedback you’ve received, or significant events in your practice.
Each account should clearly outline:
- What you learned from the experience.
- How it has improved your practice.
- How it relates to the NMC Code, focusing on themes like professionalism, safety, and effective care.
Make sure to use the approved NMC reflective account form to document these insights. Additionally, you’ll need to engage in a reflective discussion with another NMC registrant. This discussion should cover your accounts and be signed off on the designated form by the registrant.
By following these steps, you’ll ensure your reflective accounts meet the required standards while demonstrating your commitment to safe and effective nursing practice.
How can I reflect without risking patient confidentiality?
When writing reflections in healthcare, it's essential to prioritise patient confidentiality. This means removing or altering any details that could reveal a patient's identity. Avoid including names, exact dates, specific locations, or other identifiable information. Instead, use general terms and descriptions to discuss situations.
The focus of your reflections should remain on your professional growth, learning, and experiences. By doing so, you not only maintain privacy but also ensure your reflective practice aligns with ethical and legal standards.