10 Common Mistakes in Healthcare Reflective Practice
Improve reflective practice by avoiding 10 common errors: be analytical, link to standards, protect confidentiality and act on feedback.

Reflective practice is a critical part of healthcare, helping professionals analyse their experiences and improve their practice. However, many fall into common mistakes that weaken their reflections and risk non-compliance with professional standards. Here are the ten most frequent errors and how to avoid them:
- Overly Descriptive Writing: Focusing too much on what happened without analysing why or how to improve.
- Not Linking to Professional Standards: Failing to reference guidelines like the NMC Code or HCPC standards.
- Lack of Focus on Learning: Missing the opportunity to identify specific lessons or changes to practice.
- Breaching Confidentiality: Including details that could identify patients.
- Unstructured Reflections: Writing without a clear framework, leading to unfocused narratives.
- Avoiding Negative Experiences: Skipping over mistakes instead of learning from them.
- Using Complex Language: Overloading reflections with jargon or unnecessary technical terms.
- Skipping Reflective Models: Not using frameworks like Gibbs or Driscoll to guide reflections.
- Inconsistent Practice: Reflecting sporadically instead of making it a regular habit.
- Ignoring Feedback: Failing to engage peers or act on their input.
To improve, focus on concise analysis, tie reflections to standards, maintain confidentiality, and use structured models. Regular practice and peer discussions can also strengthen your reflections and meet regulatory requirements.
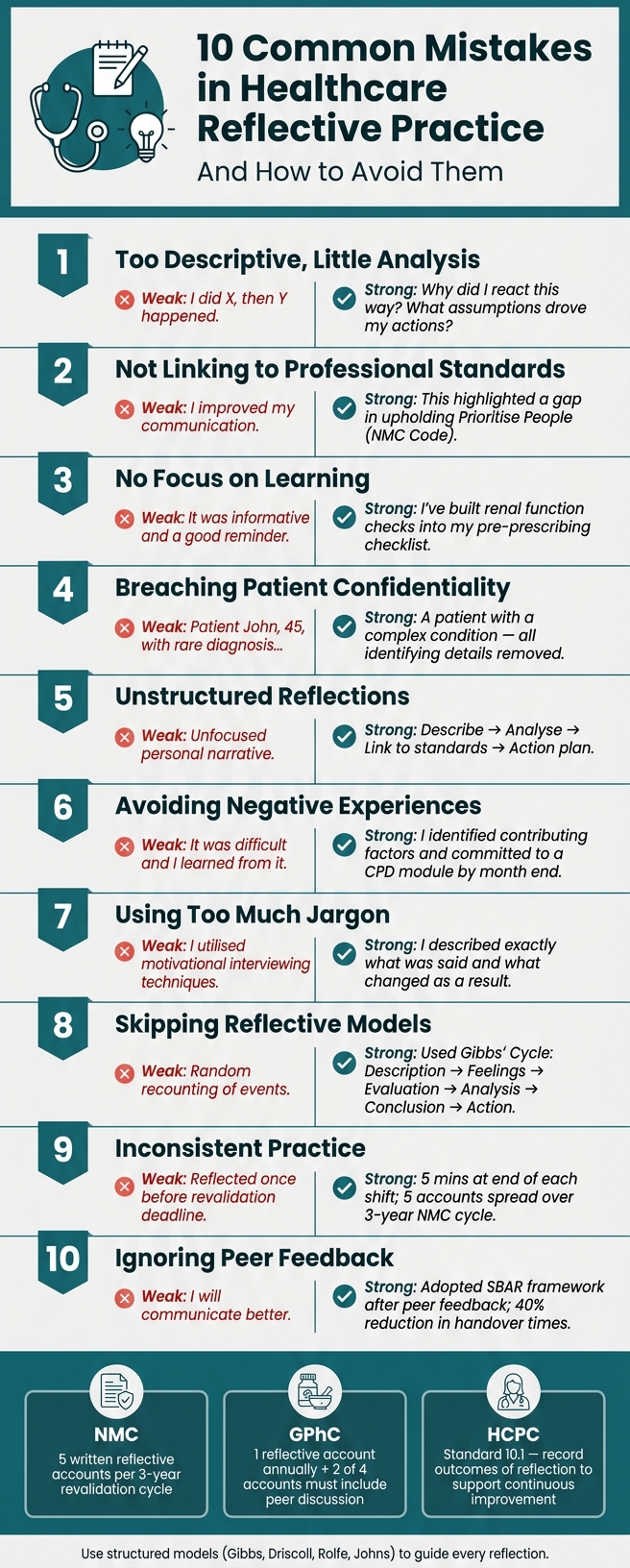
Weak vs Strong Reflective Practice: 10 Common Mistakes
The Personal Impact of Reflective Practice
sbb-itb-a476a38
1. Writing Too Descriptively with Little Analysis
One of the most frequent pitfalls in reflective practice is getting stuck in the details - describing events, settings, and actions - without digging into the reasons behind them or considering what they mean for future practice.
Cathryn Watters, Founder of Fit2Practise, explains it well:
"Many reflections remain at a narrative level: 'This happened, then I did this.' Critical reflection requires deeper questioning." [11]
While description sets the scene, it’s the analysis that reveals the why and leads to meaningful change. Revalidation Copilot highlights this difference by comparing a strong Gibbs reflection to a short story with a moral, while a weak one feels more like a police report. [9]
To avoid this, keep the descriptive part concise - just two or three sentences - and spend more time on analysis and action. Ask yourself questions like: "Why did I react the way I did? What assumptions influenced my actions? How might others have interpreted the situation?" These types of questions steer your reflection from simply recounting events to truly learning from them.
Insight is the goal of reflective practice. As Probity & Ethics points out, "The difference between a reflective statement that satisfies a regulator and one that undermines your case comes down to one thing: genuine, evidenced insight." [12] Avoid vague takeaways like "I’ll improve my communication." Instead, focus on specific, actionable changes tied to a real experience and a relevant professional standard. This depth of analysis lays a solid foundation for aligning reflections with professional expectations later on.
2. Not Aligning Reflections with Professional Standards (e.g., NMC, HCPC)
One of the biggest missteps healthcare professionals can make is failing to connect their reflections to their regulatory framework. Without directly referencing the relevant professional standards, your reflection may fall short of your regulator’s expectations.
For NMC registrants, it’s essential to link each of your five mandatory reflective accounts to a specific part of the NMC Code. The Code is organised around four themes: Prioritise people, Practise effectively, Preserve safety, and Promote professionalism and trust [1][14]. However, simply mentioning a theme isn’t enough. Your reflection must demonstrate how your experience connects to a particular aspect of the Code. As Probity & Ethics explains:
"Every NMC revalidation reflective account must identify a specific part of the NMC Code that the reflection relates to." [8]
This explicit connection ensures your reflection meets compliance requirements and fosters meaningful professional growth.
For HCPC registrants, Standard 10.1 emphasises the importance of reflective practice, stating that professionals must "understand the value of reflective practice and the need to record the outcome of such reflection to support continuous improvement" [2]. Reflective notes are also critical during CPD audits. If your reflections are vague or fail to reference specific standards, you could face challenges if your submission is reviewed.
To align your reflections with professional standards, cite specific Code numbers or themes in your accounts. For instance, instead of writing, "this experience improved my communication", try something more precise: "This experience highlighted how I was not fully upholding Prioritise People (NMC Code), particularly in how I communicated with the patient about their care options." This approach clearly ties the standard to the changes in your practice.
Avoid generalisations like describing what you "always do." Instead, focus on a specific event, identify the relevant standard, and explain the adjustments you made to your practice.
Tools such as Reflection Guide offer structured prompts based on recognised reflective frameworks, helping you align your experiences with professional standards. These prompts are tailored to support NMC revalidation, HCPC CPD, and GMC appraisals, ensuring your reflections are both compliant and meaningful.
3. Failing to Focus on Learning and Development
Healthcare professionals often document events without addressing the key question: "What did this experience change or reinforce in the way I think about my practice?" When reflections lack this critical element, they risk being purely descriptive rather than truly insightful.
"What did this experience change or reinforce in the way I think about my practice? If you cannot answer that question, your reflection is likely to remain descriptive rather than analytical." - Probity & Ethics [8]
Effective reflection goes beyond summarising events; it captures specific learning and developmental outcomes. For instance, a weak reflection might state: "I attended a training day on medication safety. It was informative and a good reminder of best practice." In contrast, a strong reflection would pinpoint the exact learning and its impact on practice: "The training made me realise I had not been consistently checking renal function before prescribing certain medications. I have since built this into my pre-prescribing checklist." This shift from general observations to actionable insights highlights professional growth.
Using vague language can signal a lack of meaningful development. Phrases that fail to articulate concrete learning outcomes provide little evidence of genuine improvement or change.
"Reflection without a concrete practice change is description, not reflection." - iatroX [6]
To ensure your reflections drive growth, end each one with a specific, actionable takeaway. Asking yourself "What do I know now that I couldn't do before?" [1] is a simple yet effective way to confirm that your reflection has moved beyond recounting events and into the realm of professional advancement.
4. Overlooking Patient Confidentiality in Reflections
Reflective practice thrives on honesty, but that openness can sometimes lead healthcare professionals to include too much detail about patient interactions. It's critical to avoid sharing information that could indirectly identify a patient, even if no names are mentioned.
This issue carries both legal and professional risks. Under GDPR, reflections that aren't anonymised might be considered personal data, meaning patients could request access to them through a Subject Access Request (SAR) [16]. Additionally, written reflections can be used as evidence in legal cases.
"Whatever is committed to a written format may be accessible to a court of law so all professional documentation, including reflections, should be written in a professional manner." - NHS England [15]
Rather than steering clear of sensitive cases altogether, focus on writing about them in a way that protects patient confidentiality. Strip out any identifying details - such as names, ages, unique diagnoses, or exact dates - and maintain a neutral, professional tone. NHS England advises:
"Ensure that everything you write is couched in professional and neutral terms. Think professional, not confessional and avoid being judgemental of yourself or others." - NHS England [15]
5. Writing Reflections Without a Clear Structure
When reflecting on experiences, especially in a professional setting, having a clear structure is absolutely crucial. Without it, reflections can easily turn into unfocused storytelling, lacking the depth and direction needed to identify key lessons or necessary changes. This is a common pitfall: reflections that seem like a personal narrative but fail to evolve into a meaningful professional analysis.
A strong reflection follows a logical progression. Start with a brief description of the experience, then touch on your emotional response and evaluate what went well and what didn’t. The heart of the reflection lies in the analysis - this is where you link your experience to nursing theory, existing research, or professional guidelines such as the NMC Code. Finally, conclude by summarising what you’ve learned and outlining a detailed action plan for improvement. This approach ensures your reflection is both insightful and aligned with professional expectations.
"The strength of Gibbs' model lies in its progression from description through analysis to action. This ensures that reflection leads to concrete learning and practice change, rather than remaining at the level of description." - Dr Sarah Mitchell, Senior NHS Appraiser [10]
Two popular frameworks can help structure reflections effectively. Gibbs' Reflective Cycle, with its six stages, is ideal for tackling complex scenarios like clinical incidents or ethical challenges. On the other hand, Driscoll’s "What? So What? Now What?" model offers a simpler format, perfect for quick reflections after a shift [9]. The choice between these models depends on the complexity of the situation, but both highlight how structure enhances the quality of reflective practice.
When writing, keep the description concise - two or three sentences are enough. Focus most of your effort on the analysis and action plan. Be specific in your action plan; for example, instead of saying, "I will improve my communication", outline concrete steps like attending a communication workshop or reviewing relevant sections of the NMC Code. This level of detail ensures your reflection translates into meaningful professional growth.
6. Avoiding Difficult or Negative Experiences
It's human nature to shy away from uncomfortable situations, but skipping over negative experiences during reflective practice can seriously limit professional development. Some professionals tend to avoid delving into these moments or resort to vague reflections like, "It was a difficult situation, and I learned from it." Unfortunately, such statements often fail to provide the level of detail regulators require.
Confronting challenging experiences is just as important as ensuring your reflections meet professional standards.
Regulatory bodies such as the NMC, GMC, and HCPC place a high value on the ability to reflect on mistakes. They see this as a hallmark of professional self-awareness. As Probity & Ethics explains:
"Insight - genuine understanding of what went wrong, why, and what has changed as a result - is one of the primary indicators that a professional poses a reduced risk to patients and the public in the future." - Probity & Ethics [12]
Avoiding tough reflections not only stunts your growth but might also raise concerns about your ability to learn from mistakes. A practitioner who downplays issues or provides generic reflections risks appearing as though they lack the depth needed for meaningful growth.
Here’s a comparison to illustrate the difference between weak and strong reflections on a negative experience:
| Feature | Weak Reflection | Strong Reflection |
|---|---|---|
| Focus | Vague regret ("I regret the situation") | Specific analysis of the failure and its impact |
| Responsibility | Shifts blame externally | Honest acknowledgement of personal accountability |
| Outcome | Generic promises ("I'll do my best") | Concrete actions, like completing a CPD course or implementing new protocols |
| Depth | Surface-level description of the event | Detailed exploration of causes and challenged assumptions |
When reflecting on a mistake, avoid falling into the trap of self-blame. Instead, focus on identifying the factors that contributed to the issue. These could include workload challenges, communication breakdowns, or even equipment failures. The goal here isn’t to make excuses but to understand the situation fully so you can determine what needs to change.
Turn your insights into actionable steps with clear deadlines. For example, instead of saying, "I’ll be more careful in the future," commit to something measurable like, "I’ll complete the Trust’s medication safety module by the end of the month."
Taking this approach to difficult experiences reinforces the importance of depth, accountability, and a commitment to improvement in reflective practice.
7. Using Too Much Jargon or Complex Language
In healthcare, clinical terminology has its place, but overloading your reflective practice with it can blur the true lessons you've learned. Complex language can make your reflection feel more like a formal report than a personal account of growth.
Probity & Ethics sums it up well:
"Generic language - phrases like 'I will always try to do my best' or 'I take patient care very seriously' that could apply to any professional in any situation [undermine reflective statements]." [12]
When your writing is filled with unexplained acronyms, technical terms, or overly formal language, it becomes harder for others to follow. The UK Clinical Pharmacy Association recommends spelling out acronyms in full the first time they appear, ensuring your reader has the context they need [17].
Using straightforward language helps simplify complex ideas and highlights the personal nature of your reflection. Regulators prefer reflections that feel authentic and grounded in real experiences. Instead of saying, "I demonstrated effective patient-centred communication utilising motivational interviewing techniques", describe a specific moment. Share what was said, how it impacted the situation, and what you learned. This kind of detail makes your reflection more relatable and meaningful.
"A good Gibbs reflection reads like a short story with a lesson. A bad one reads like a police statement." - Revalidation Copilot [9]
The key is to keep your language concise and genuine. Here's a quick test: if your reflection could apply to any healthcare professional in any scenario, it’s too generic. Focus on unique, real events and insights. In the next section, we'll explore how reflective models can help bring even more clarity to your writing.
8. Not Using a Recognised Reflective Model
Reflection without structure can easily turn into a simple recounting of events, offering little in terms of insight or growth. A recognised reflective model provides a clear framework, ensuring your thoughts lead to meaningful conclusions and actionable steps.
"Reflective models give you a framework so that your reflection goes somewhere useful rather than just going round in circles." - Amelia Scarlett, Learnera [7]
In UK healthcare, several reflective models are commonly used, each suited to different scenarios. For instance, Gibbs' Reflective Cycle is a detailed six-stage process (Description, Feelings, Evaluation, Analysis, Conclusion, and Action Plan) that’s ideal for unpacking complex clinical incidents or emotionally charged experiences. On the other hand, Rolfe's Framework (What? So What? Now What?) offers a simpler approach, making it perfect for quick reflections, such as at the end of a shift, or for those just starting to develop reflective habits. Schön's Model introduces the distinction between reflection-in-action (adjusting in the moment) and reflection-on-action (analysing events after they occur) [7]. These structured methods tie in well with earlier advice on writing reflections that are clear and concise.
Whichever model you choose, consistency is key. The Action Plan stage, in particular, is crucial. Regulatory bodies like the NMC, which requires five written reflective accounts over a three-year revalidation period [1], place significant emphasis on how you plan to act differently as a result of your reflection. Tools like Reflection Guide are designed around frameworks such as Gibbs, Driscoll, and Kolb, ensuring you don’t overlook the analytical elements that are often the most impactful.
9. Reflecting Inconsistently or Infrequently
Staying consistent with reflection ensures timely and detailed insights, paving the way for continuous improvement. Unfortunately, many healthcare professionals fall into the habit of reflecting sporadically, often delaying documentation until the revalidation deadline looms. By then, memories fade, and crucial details - like a patient’s exact words or key turning points - are often lost.
"The sooner you reflect on your activity, the more truthful to the event your recollection will be, so make it part of your regular routine." - Royal College of Nursing [3]
In the UK, regulatory bodies place a strong emphasis on consistent reflection. Nurses and midwives, for instance, are required to complete 5 written reflective accounts over a three-year revalidation cycle [3]. Pharmacists and pharmacy technicians, on the other hand, need to submit 1 reflective account annually under GPhC revalidation requirements [5]. Spreading these reflections throughout the cycle not only makes the process more manageable but also ensures richer, more meaningful accounts.
"An account written in the week before renewal will almost always be thinner than one written with some distance from the experience." - LUDA Partners [5]
Incorporating reflection into your routine doesn’t have to be a time-consuming task. For example, try spending just five minutes at the end of each shift jotting down three key takeaways from your day. If writing feels like a hurdle, record a quick voice note and transcribe it later. The goal is to capture the experience while it’s still vivid, then revisit it later using structured models like Gibbs or Driscoll to analyse it further.
Tools like Reflection Guide can streamline this process, allowing you to log your thoughts quickly and develop them into detailed drafts.
"Small, regular reflections make a bigger difference over time than occasional formal reviews." - Amelia Scarlett, Learnera [7]
Setting a monthly reminder to review and document recent experiences can help turn reflection into a natural habit rather than a last-minute chore. Beyond meeting revalidation standards, regular reflection fosters ongoing professional growth and development.
10. Ignoring Feedback and Peer Input
Engaging with peers is essential for meaningful reflection, as it can help reveal perspectives you might otherwise miss. Reflecting in isolation has its limits because you’re confined to what you already know. Peer input, on the other hand, challenges assumptions, highlights blind spots, and encourages deeper, more critical thinking instead of surface-level descriptions [1][11]. However, many healthcare professionals treat reflection as a solitary activity, overlooking the value of collaborative input.
This isn’t just a missed opportunity - it’s a regulatory necessity. The NMC requires a reflective discussion with another registrant as part of revalidation [1], while the GPhC mandates that two of your four annual reflective accounts must involve peer discussion [6]. Skipping this step not only weakens your reflection but could also jeopardise your revalidation.
"To be effective, reflection requires you and your colleagues to be open and honest with each other, without fear of being blamed." - The HCPC [2]
One common mistake is failing to act on feedback in a meaningful way. For example, instead of vaguely noting, "I will communicate better", it’s more effective to pinpoint specific actions. In April 2026, a nurse received feedback from a senior colleague about overly lengthy handovers. Using this input, they adopted the SBAR framework (Situation, Background, Assessment, Recommendation), which led to a 40% reduction in handover times and clearer communication for the incoming shift. This improvement was documented as a reflective account aligned with the NMC Code’s "Practise Effectively" theme [13].
Even if you don’t have colleagues nearby who are also registrants, you can still engage in peer discussions by connecting with professional networks or speciality groups outside your workplace [1]. The critical step is to document the impact of the feedback you receive. Record what was said, the changes you made, and the outcomes that followed [5]. This practice not only strengthens your reflective process but also lays the groundwork for continued growth and improvement.
How to Improve Your Reflective Practice
Improving your reflective practice doesn’t require a complete overhaul - small, focused adjustments can make a big difference. Many of the common mistakes in reflection come from habits that are easy to slip into but just as easy to correct once you know what to focus on. A good starting point is to choose a reflective framework that fits your needs.
Start with structure. A simple four-part framework can help organise your thoughts: briefly describe the experience, highlight what you learned, connect it to a specific professional standard, and outline one actionable change. Keep in mind, the description is only the beginning - the real value lies in your analysis. Try asking yourself, "How has this experience influenced or reinforced my thinking?" rather than recounting the event step by step [8].
Pick the right reflective model. Different models work best for different situations:
- Rolfe's "What? So what? Now what?" is ideal for quick reflections, like at the end of a shift or during initial practice.
- Gibbs' Reflective Cycle is better suited for more complex scenarios, such as clinical incidents, where you need to explore emotions, evaluations, and future actions.
- Johns' Model provides a structured way to reflect on ethically challenging situations, such as end-of-life care.
There’s no one-size-fits-all solution - what matters is choosing a model you feel comfortable using consistently.
"The professionals who keep improving over the course of a career are not necessarily the ones who attended the most courses. They are the ones who kept asking honest questions about their own practice, and then did something with the answers." - Amelia Scarlett, Learnera [7]
A structured approach like this also helps align your reflections with professional standards. For example, if you’re reflecting on patient safety, you might link your insights to the "Preserve Safety" principle in the NMC Code. Keep it simple: explain the connection in plain language. If you can’t sum it up in one sentence, you might be overthinking it [4][8].
Lastly, always protect patient confidentiality. Avoid including names or specific details, and consider using tools with built-in privacy checks to ensure your reflections are anonymised before you finalise them.
Conclusion
Reflective practice, when done with intention and care, has the potential to drive meaningful professional growth. It’s not just about meeting requirements; it’s about fostering genuine improvement in the quality of care and strengthening your professional standing.
The challenges outlined earlier - like over-reliance on descriptive writing or inconsistent habits - all share a common flaw: they undermine the true purpose of reflection. As the Royal College of Nursing explains:
"Reflection helps us to think about, plan and deliver high quality and safe care to our patients/clients." [1]
When reflection is rushed or treated as a tick-box exercise, its value is diminished. Poorly executed reflections can even risk your revalidation or harm your professional credibility.
The good news? These pitfalls are avoidable. Start by selecting a reflective model that fits your needs. Focus on analysis rather than just recounting events, connect your insights to professional standards, and be open about areas for improvement. As the HCPC advises:
"Reflection should focus on what is in your control, rather than replaying past mistakes. It should leave you feeling positive and hopeful, rather than negative about your own abilities." [2]
Striking this balance between honesty and constructive thinking is what sets effective reflection apart. By consistently practising structured and thoughtful reflection, you not only meet regulatory standards but also elevate the care you provide. Small adjustments can turn reflection into a tool for continuous improvement, helping you grow both personally and professionally.
FAQs
How do I make my reflection more analytical?
To deepen your reflective analysis, steer clear of simply recounting events. Instead, apply structured models such as Gibbs’ Reflective Cycle to link your experiences with professional standards, research, or theoretical frameworks. Consider questions like: What assumptions did this challenge? What lessons emerged from the experience? Aim to pinpoint the factors that influenced the situation and ensure your reflection results in clear, actionable steps to enhance your practice.
Which reflective model should I use for my situation?
When it comes to reflective practice, there’s no one-size-fits-all model. The key is to pick one that fits your needs and style. For something straightforward, Driscoll’s three-stage model (What, So what, Now what) offers a quick and practical approach. If you’re looking for a more in-depth framework, Gibbs’ six-stage model is a solid choice, as it encourages you to explore emotions and map out detailed action plans. Ultimately, the best model is the one that clearly shows your learning process and aligns with the standards of your profession.
How can I write honestly without breaching confidentiality?
To write transparently while respecting confidentiality, shift your focus to what you’ve learned and how it will shape your future actions, rather than recounting specific cases. Ensure anonymity in your notes by leaving out any names, dates of birth, addresses, or identifiable locations. Information is considered anonymised only if individuals cannot be identified, even when cross-referenced with other data. The purpose of your reflection is to showcase professional growth and understanding - not to provide a detailed account of events.