GMC Appraisal Reflection: What You Need to Include
Make GMC appraisal reflections short and anonymised: state what happened, the learning, and the change with a simple template.
A GMC appraisal reflection only needs to do 3 things: say what happened, say what I learned, and say what I changed. If those points are clear, brief, and anonymised, the entry is usually fit for appraisal.
In practice, I keep each note focused on:
- The activity: what I did, with Month/Year and a short setting note
- The learning: the main point I took from it
- The action: what I changed, or what I will do next
- The link: how it fits my PDP or Good Medical Practice
- Confidentiality: no names, no exact dates, no details that could identify a patient or colleague
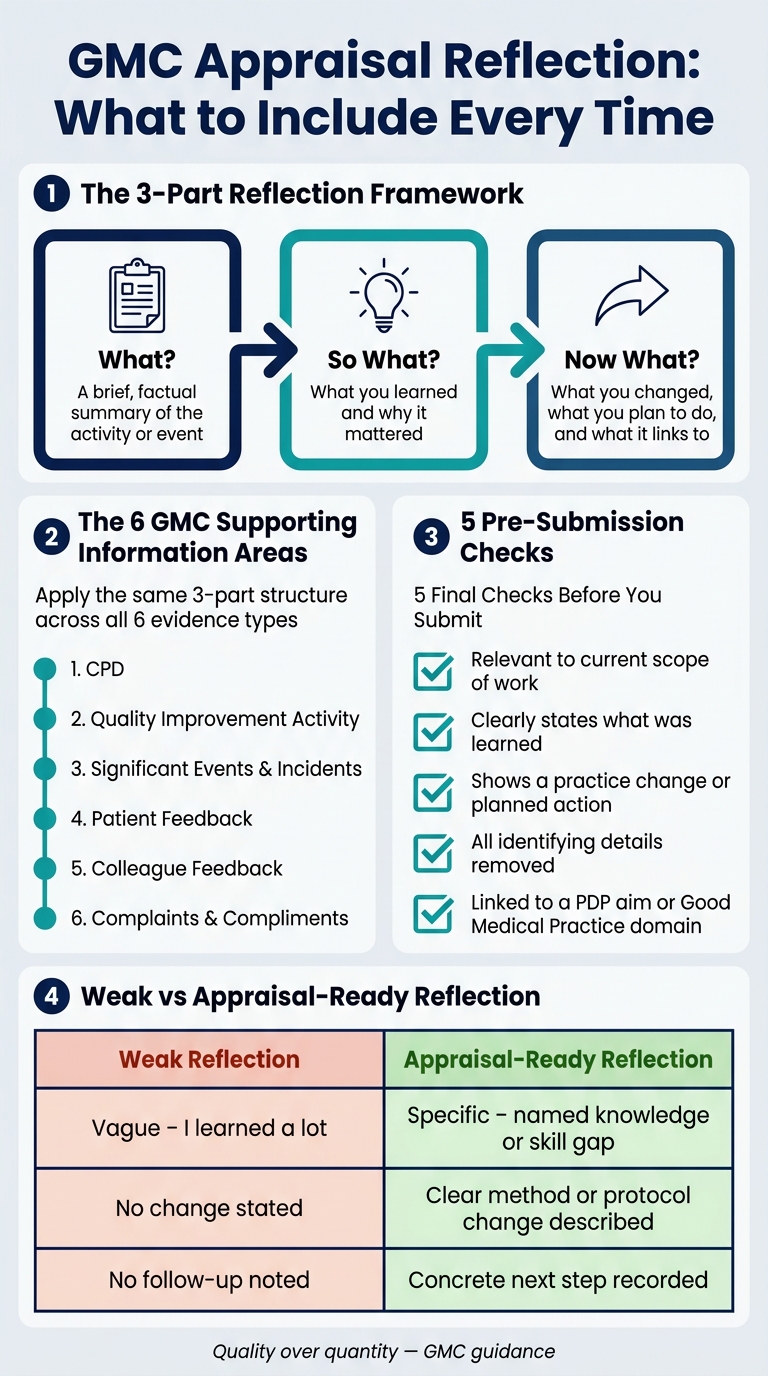
The same approach works across all 6 GMC supporting information areas:
- CPD
- Quality improvement activity
- Incidents
- Patient feedback
- Colleague feedback
- Complaints and compliments
A short reflection is often better than a long one. The GMC focus is on quality over quantity, so I aim for a few clear entries instead of a long record with no learning or action.
Here’s the simplest way to think about it:
| Part | What I include |
|---|---|
| What? | A brief, factual summary of the activity or event |
| So what? | What I learned and why it mattered |
| Now what? | What I changed, what I plan to do, and what it links to |
I also do a final check before I submit anything:
- Is it tied to my current work?
- Does it show clear learning?
- Does it show a change or next step?
- Is it anonymised?
- Does it link to a PDP aim or GMC domain?
If I can answer yes to all 5, the reflection is usually ready to use.
GMC Appraisal Reflection Framework: What to Include Every Time
Doing 'Reflection' for Medical Appraisal 🧠 | Doctors Appraisal UK | Medical Appraisals
sbb-itb-a476a38
What to include in every reflective entry
Write enough so an appraiser can see the activity, the learning, and the change straight away. Every reflective entry should cover those three points.
The GMC puts it simply:
"A reflective note does not need to capture full details of an experience. It should capture learning outcomes and future plans." - General Medical Council [4]
A simple way to keep your entry on track is: What? So what? Now what? [4] It keeps things clear and makes the reflection easy to read.
Describe the activity briefly and factually
Keep this part short. Say what the activity was, give the date as Month/Year only, such as April 2026, and note the general setting, like a GP practice, acute medical ward, or outpatient clinic. You do not need full case details. Give just enough background to make the learning point clear, not the whole case history.
State the learning and why it mattered
Be specific about what you learned. That could be new clinical knowledge, a communication point, or a problem in a process. Then link it to why it mattered, such as a domain of Good Medical Practice, your current Personal Development Plan (PDP), or the effect on patient care.
Stronger reflection is precise. It names the learning point clearly, for example a gap in your knowledge or a communication issue that affects patient care.
Show the practice change and next step
Say clearly what has changed already, or what you will do next. This could mean updating a protocol, changing how you explain something to patients, arranging further CPD, or adding a new action to your PDP. Reflection should drive change in practice and CPD [5], so this action step shows how the learning has shaped your work. Use the same structure for CPD, incidents, feedback, and complaints.
What to include for each type of GMC supporting information
Use the same three-part structure for each evidence type, but shift the emphasis to fit where the learning came from. The framework stays the same. What changes is the main question you need to answer.
CPD and quality improvement activity
For CPD, explain why you chose the activity, note two or three main learning points, and say exactly how it changed your practice [3]. The key thing here is the effect on your day-to-day work, not a summary of the course.
For QI, set out the findings, what changed, and whether that change improved practice or still needs more work [1][3]. A handy way to sense-check your reflection is the Stop, Start, Continue framework: what will you do now that you were not doing before, what will you keep doing because it reflects best practice, and what will you stop because it no longer reflects best practice [3]?
Significant events, incidents, and complaints
Start with a short factual summary of the event or complaint. Then explain your role, your part in the review, the contributory factors, and the exact actions taken at individual or system level to help prevent it happening again [1][2]. Keep the emphasis on reducing risk and changing systems, not retelling the whole incident.
If you were personally named in a significant event or serious incident, you must sign a declaration and provide a reflective commentary for each one [1].
Patient feedback, colleague feedback, and compliments
Compare the feedback with your own view of your practice, spot the main themes, and record the change you will make or have already made [1]. Instead of reacting to one-off comments, look for patterns in communication, access, or teamwork, then name the next step in plain terms [1][3]. Compliments matter too. They can show what you’re doing well. Note what behaviour or approach led to the positive response and how you’ll keep that standard in place [1].
Use the table below as a quick drafting check.
| Evidence type | Primary focus | Key question to answer |
|---|---|---|
| CPD | Knowledge and skill update | What will I do now that I wasn't doing before? |
| Quality improvement | Process and outcomes | Have the changes I made improved practice? |
| Significant events | Risk and system safety | What contributory factors led to this, and how can we prevent recurrence? |
| Feedback | Professionalism and communication | How does the way others see me differ from how I see myself? |
How to document reflection safely and proportionately
Once you've written the learning and action, give the entry a final check for anonymity and proportion. Think of every entry as a professional record that could be disclosed. For appraisal, include only the detail that earns its place.
Remove patient-identifiable and colleague-identifiable details
The main rule is simple: do not include names, NHS numbers, full dates of birth, addresses, or any mix of details that could identify someone indirectly.
Instead of trying to redact an original document - and risking that something slips through - write a new, anonymised summary that stays focused on the learning and the action [6]. Broad descriptions usually work best, such as "an adult patient," "a paediatric case," or "a multidisciplinary team" [4].
That way, you protect identities without losing the point of the reflection. The note still works for appraisal, but it doesn't carry extra detail that doesn't need to be there.
Keep the tone honest, balanced, and concise
State the learning and the next step plainly. Leave out anything that doesn't change the appraisal point. If the event brought up strong emotions, it can help to draft the entry and come back to it 24 hours later before reading it again [4]. That pause often helps keep the tone calm and professional.
Try to focus on two or three meaningful changes, not a blow-by-blow account. If you're not sure the tone lands well, ask a trusted colleague to look it over for tone and brevity [4].
Use a clear structure or guided template
Using the same structure each time makes the note shorter, more proportionate, and focused on action. It also makes the entry easier to review at appraisal.
Use these checks before you complete the template below.
A simple template for your next GMC appraisal reflection
Recommended headings for each entry
Use this template to record the activity, what you learned, and what changed in your practice in one short entry. The aim is simple: keep each reflection short, clear, and easy to review.
Use these seven headings for a consistent reflective entry.
| Heading | What to write |
|---|---|
| Activity title and type | Name the event and its category, such as CPD, Significant Event, or Patient Feedback |
| Context | A one-sentence anonymised summary of the activity or event |
| Why it mattered | Why the experience stood out and why it was worth reflecting on |
| Key learning | The specific knowledge, skill, or insight you gained |
| Practice impact | How this changes, shapes, or reinforces the way you work |
| Actions taken/planned | Clear next steps, such as updating a protocol, booking a course, or revising a process |
| PDP or Good Medical Practice link | Which Personal Development Plan aim or Good Medical Practice domain this connects to |
Weak reflection vs appraisal-ready reflection: a comparison
A strong entry does three things: it states the learning clearly, shows the effect on practice, and includes a next step. That’s what an appraiser needs to spot quickly.
The table below shows the gap between a vague note and a reflection that is fit for appraisal.
| Feature | Weak Reflection | Appraisal-Ready Reflection |
|---|---|---|
| Learning | Vague - "I learned a lot" or "It was interesting" | Specific - "I learned a new local pathway" |
| Practice impact | Absent - "No change stated" | Clear - "I will now use the DESC method to resolve conflicts in the MDT" |
| Action plan | Missing - no follow-up noted | Concrete - "I have created a new referral template for the practice" |
| Confidentiality | Includes names, initials, or specific dates | Fully anonymised - refers to "a middle-aged patient" |
| Linkage | Isolated entry, no broader connection | Linked to PDP goals or specific Good Medical Practice domains |
Final checks before you submit your reflection
Before you mark an entry as complete, run through these questions. If the answer is yes each time, it’s ready to submit.
- Is it relevant to your current scope of work?
- Does it clearly state what you learned?
- Does it show a change in practice or a planned action?
- Are all identifying details removed?
- Is it linked to a PDP aim or Good Medical Practice domain?
FAQs
How long should a GMC reflection be?
The GMC does not set a minimum or maximum length for reflective entries. The focus is on quality, not word count.
Keep your reflection concise and ready for appraisal. Cover the key points:
- what happened
- why it matters to you
- what action you took, or plan to take
Leave out extra detail, and do not include patient-identifiable information.
Can I use the same reflection structure for every evidence type?
No. The GMC does not ask for one set format for every reflection.
You can use the structure or reflective model that fits the way you learn and the activity you’re writing about. That might be a simple framework like What, So what, Now what, or a different approach that works better for you.
What matters most is this: show how the activity changed your practice and affected patient care.
What details should I leave out to keep a reflection anonymised?
Leave out any detail that could point to a patient, colleague or any other third party. Just taking out names, ages and addresses often isn’t enough. Other bits of information can still make someone identifiable.
Skip full case histories and extra detail you don’t need. Put the focus on what you learned, how it changed your practice, and what you plan to do next. If the information is sensitive, keep the written note general and talk through the detail with your appraiser in person.