5 Reflective Models Every Healthcare Student Should Know
Five practical reflective models for healthcare students that improve clinical judgement, CPD and everyday decision-making.

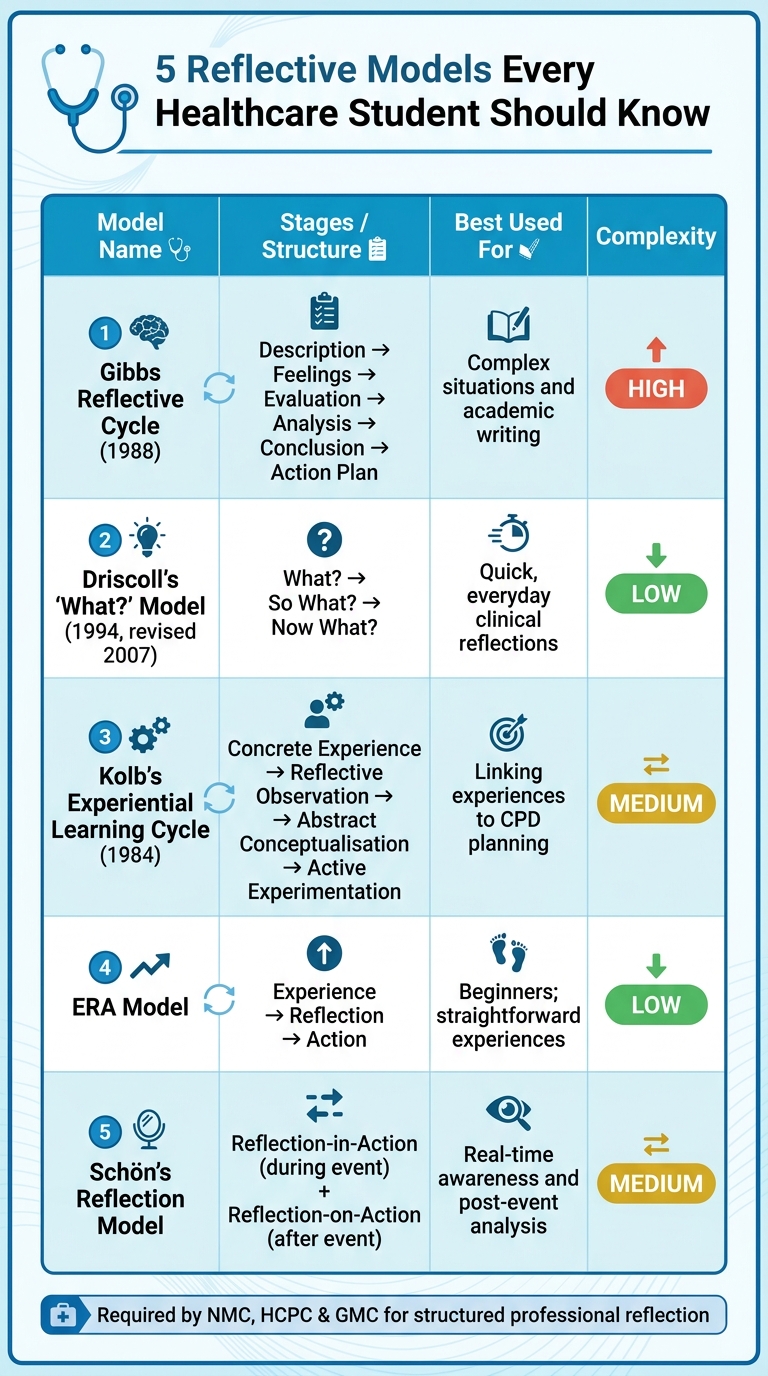
Reflective practice is a key skill for healthcare students in the UK, helping to improve decision-making and patient care. Professional bodies like the NMC, HCPC, and GMC require structured reflections as part of training and revalidation. Using reflective models provides a clear framework for analysing experiences and learning from them. Here are five widely used models:
- Gibbs Reflective Cycle: A six-step process focusing on description, feelings, evaluation, analysis, conclusion, and action planning. Ideal for in-depth academic reflections.
- Driscoll's 'What?' Model: A simpler framework with three questions: What? So what? Now what? Useful for quick reflections in clinical settings.
- Kolb's Experiential Learning Cycle: A four-stage loop (experience, observation, conceptualisation, and experimentation) that links experiences to continuous learning.
- ERA (Experience–Reflection–Action) Model: A straightforward three-step process for fast-paced environments.
- Schön's Reflection-in-Action and Reflection-on-Action: Combines real-time adjustments with post-event analysis for deeper insights.
Each model suits different situations, from quick reflections to detailed academic work or clinical decision-making. Choosing the right one depends on your needs and the context of your experience.
5 Reflective Models for Healthcare Students: Quick Comparison Guide
Models of reflection for reflective writing
sbb-itb-a476a38
1. Gibbs Reflective Cycle
Professor Graham Gibbs introduced this model in 1988, and it's become a staple in healthcare education across the UK. Although initially created for nursing, it’s now widely applied in fields like medicine, physiotherapy, and midwifery [3].
What sets this model apart is its cyclical design, encouraging you to revisit and rethink experiences repeatedly. This ongoing process helps clarify events and their underlying causes, making it a valuable tool not just for academic tasks but also for professional growth. Its structured approach ensures a clear path to meaningful reflection.
"This cyclical model, as opposed to a linear one, emphasizes the importance of continuously revisiting experiences, analyzing them from different angles, and using the insights gained to inform future actions and improve decision-making." - Simply Psychology [3]
The cycle is broken into six stages:
- Description: A factual account of what happened.
- Feelings: An exploration of your emotional reactions.
- Evaluation: Identifying what went well and what didn’t.
- Analysis: Connecting the experience to relevant theories or guidelines.
- Conclusion: Extracting key lessons from the experience.
- Action Plan: Creating SMART goals (Specific, Measurable, Achievable, Relevant, Time-bound) for future improvement [3][4].
In nursing assignments, the Analysis stage often carries significant weight, sometimes making up to 40% of the grade. On the other hand, the Description stage should be concise, using only 10–15% of the word count to set the scene effectively. A well-developed analysis not only enhances your reflection but also demonstrates deeper critical thinking. Remember to use pseudonyms to ensure compliance with data protection and professional standards [4].
2. Driscoll's 'What?' Model
John Driscoll introduced his model in 1994, refining it in 2007 to cater specifically to healthcare professionals [5]. Rooted in Terry Borton's 1970 framework, this model revolves around three straightforward questions: What?, So what?, and Now what?. This simplicity has earned it the alternative name, the Borton/Driscoll Model [6].
Compared to Gibbs' six-stage structure, Driscoll's model is quicker and easier to apply, making it ideal for busy clinical environments where time for reflection is limited.
"Reflection isn't merely a case of looking over one's shoulder - reflection is about looking at experience, learning the lessons, and transferring them forward to practice." - Eloise Doyle [5]
Here’s how the three stages unfold:
- What?: This step involves objectively recounting the event. What happened? Who was involved? What actions did you take?
- So what?: Next, you explore the significance of the event. How did it make you feel? What was its impact on the patient, the team, or yourself?
- Now what?: Finally, you identify actionable steps. This might include seeking additional supervision, improving your approach to specific tasks, or pursuing further training [5].
While the model's simplicity makes it accessible, it can sometimes lead to shallow reflections if not approached thoughtfully. However, it’s particularly effective for capturing quick insights after incidents or near-misses.
One study involving 130 BSN students revealed that structured reflective practices significantly improved clinical reasoning for 90% of participants [7]. This highlights the importance of engaging deeply with each question, ensuring the reflection goes beyond surface-level observations.
3. Kolb's Experiential Learning Cycle
David Kolb developed his Experiential Learning Theory in 1984, building on the ideas of Dewey, Lewin, and Piaget [8]. Unlike simpler models like Gibbs' or Driscoll's, which focus on individual events, Kolb's cycle transforms experiences into testable theories, creating a continuous learning process. This approach emphasises refining knowledge through repeated application and reflection.
The cycle consists of four interconnected stages: Concrete Experience (direct involvement in an event), Reflective Observation (thinking about the experience), Abstract Conceptualisation (forming insights or theories), and Active Experimentation (applying what you've learned to test new methods) [8]. These stages repeat in a loop, making learning an ongoing process.
"Learning is the process whereby knowledge is created through the transformation of experience." - David Kolb [8]
For example, imagine your first attempt at drawing blood is unsuccessful. This experience leads you to reflect on what went wrong, adjust your technique (like changing the needle angle), and then test the new approach. This process illustrates how engaging with all four stages can improve both technical skills and clinical reasoning - essential in healthcare [8].
It's important to identify which stage of the cycle you naturally gravitate towards. For instance, if you're action-oriented but skip reflection, you might miss valuable insights. On the other hand, if you tend to overanalyse without acting, seeking more hands-on opportunities could help you grow. Striking a balance across all stages ensures a more rounded approach to learning [8].
Kolb also described four learning styles - Diverging, Assimilating, Converging, and Accommodating - each tied to how individuals process experiences [8][9]. Recognising your preferred style can highlight areas for improvement and help you approach challenges more effectively.
Think about how Kolb's cycle integrates with your reflective practice. It can serve as a guide for continuous improvement, helping you refine both your skills and your clinical judgement.
4. ERA (Experience–Reflection–Action) Model
The ERA model simplifies the process of reflective practice, making it ideal for fast-paced clinical environments. Unlike Kolb's more detailed cycle, the ERA model breaks reflection into three straightforward stages: Experience, Reflection, and Action [10]. It functions as a continuous loop - starting with a specific clinical event (whether positive or negative), moving on to reflection on the event and your feelings about it, and finally deciding on actions to take. This then leads to a new experience, restarting the cycle [10].
"Individual responses to an experience vary. This action will result in another experience and the cycle will continue." - Cambridge University Libraries [10]
For instance, imagine a student nurse who nearly administers an incorrect dose of medication. This incident prompts them to reflect on what went wrong and implement a strict double-checking protocol moving forward [5].
The simplicity of the ERA model makes it easy to adapt to different situations, providing a practical starting point for reflective practice [11].
5. Schön's Reflection-in-Action and Reflection-on-Action
Donald Schön introduced a model of reflection that stands out by incorporating two distinct modes: one that happens during practice and another that occurs afterwards. This approach bridges immediate learning with deeper, retrospective insights, making it particularly versatile.
Reflection-in-Action takes place in the moment - it’s about thinking and adjusting while actively engaged in a situation. Picture a student nurse interacting with a distressed patient's family. If the father responds angrily to routine reassurance, the nurse might pause, assess the situation, and adapt their tone and approach instantly. As La Trobe University puts it, this involves "self-awareness of your own thinking and emotional reactions", allowing for better judgments in real time [12].
Reflection-on-Action, on the other hand, happens after the fact. This mode involves looking back to analyse what occurred, enabling more profound learning. According to the University of Hull, "the role of reflection-on-action is not only one of learning and informing action, but also the building of theory" [13]. In practice, this means reviewing past events to identify gaps in knowledge, question assumptions, and refine future actions.
Here’s a quick comparison of the two modes:
| Reflection-in-Action | Reflection-on-Action | |
|---|---|---|
| Timing | During the event | After the event |
| Primary Focus | Immediate decision-making | Analysis and future planning |
| Outcome | Adjust actions on the spot | Build knowledge and improve future practice |
To make the most of Schön’s model, try setting aside 15–20 minutes each day during placements. Use this time to reflect on what surprised you, what worked well, and what you might change next time. Over time, this habit strengthens your ability to think on your feet, making reflection-in-action more intuitive.
Conclusion
Each reflection model has its strengths, and understanding when to use each one can make a noticeable difference in your practice. Driscoll and ERA are ideal for quick, everyday reflections or for those just starting out. Gibbs is particularly useful for detailed academic work, while Kolb helps tie experiences directly to your continuing professional development (CPD). On the other hand, Schön stands out in clinical environments where immediate decision-making and later analysis are both critical.
Selecting the right model doesn’t have to be complicated. As one expert puts it:
"Different people will be drawn to different models depending on their own preferences... The important part is that it works - if it doesn't then you may need to move on and try something else." [10]
Here’s a quick-reference table to help you decide:
| Model | Best Used For | Complexity |
|---|---|---|
| Driscoll | Quick, everyday clinical reflections | Low |
| ERA | Beginners; straightforward experiences | Low |
| Kolb | Linking experiences to CPD planning | Medium |
| Gibbs | Complex situations and academic writing | High |
| Schön | Real-time awareness and post-event analysis | Medium |
In healthcare, reflection is more than just a professional obligation; it’s a way to align your experiences with learning and practice. Professional bodies like the NMC, HCPC, and GMC require reflections to be structured, backed by evidence, and anonymised to maintain patient confidentiality [1][2].
Tools like Reflection Guide make this process easier. With frameworks like Gibbs, Driscoll, Kolb, and ERA built in, it offers guided prompts and privacy checks to ensure sensitive information is flagged before saving or exporting. Whether you’re working on NMC revalidation, HCPC CPD, or a GMC appraisal, it helps you create polished, professional reflections that meet the required standards. You can even start for free, making it simple to dive into reflective practice right away.
FAQs
Which reflective model should I use for my placement today?
Gibbs' Reflective Cycle is an excellent framework to use for your placement today. It walks you through six key stages: description, feelings, evaluation, analysis, conclusion, and action plan. This step-by-step process is especially useful when reflecting on clinical experiences, as it helps you pinpoint what went well, what could be improved, and how to enhance your practice moving forward.
How do I keep patient information anonymous in reflections?
To protect patient confidentiality in your reflections, ensure identifying details are removed or altered. Avoid including specific names, dates, locations, or any unique traits that might reveal someone's identity. Instead, use methods like generalisation or data masking to maintain privacy while keeping the reflection meaningful. The aim is to ensure the information remains untraceable, preserving the individual's anonymity throughout your reflective practice.
How can I make my reflection more critical, not just descriptive?
To bring more depth to your reflection, shift your focus from simply recounting events to critically analysing them. Look closely at your assumptions, emotions, and the motivations behind your actions.
Consider asking yourself questions such as: What led to this outcome? What factors shaped my reaction? How might I approach this differently next time? This method not only enhances self-awareness but also provides meaningful lessons to apply in the future.